
An association between ankyloglossia and periodontitis has not been previously reported. In the presented series of clinical cases, three sisters are described, each of whom had ankyloglossia and localized periodontitis in the region of the molars and incisors. The simultaneous occurrence of both conditions in the family suggests that further study of genetic factors that may simultaneously influence the pathogenesis of both disorders may be warranted.

Ankyloglossia (AG), commonly referred to as tongue-tied tongue, is a congenital oral disease characterized by an abnormally thick, tight, or short frenulum of the tongue, resulting in limited tongue motility. Ankyloglossia develops during the developmental period of the embryo, as a result of insufficient degeneration of the lingual frenulum. The condition varies in severity and is usually associated with functional limitations in infants, including difficulty breastfeeding, atypical swallowing habits leading to malnutrition, and impaired speech later in life.
The prevalence of ankyloglossia has been reported to generally range from 2% to 4%, although prevalence as high as 10% has also been observed. This difference may be due to the lack of a universal definition of the disease or conflicting diagnostic criteria. The exact etiology of ancloglossia has not been fully elucidated, it is assumed that genetic factors underlie the disease. A variety of sources describe familial inheritance of the disease from the heterozygote, most likely due to the wide variation in the severity of ankyloglossia and the lack of a generally accepted classification system, which has led to the use of multiple systems using different diagnostic criteria.
Periodontitis is an inflammatory disease caused mainly by the accumulation of plaque, which leads to the progressive destruction of tooth-supporting structures and ultimately to tooth loss.
Historically, periodontitis has been divided into four different categories according to the clinical presentation, which varied according to the severity of the disease (chronic, aggressive, necrotizing, and periodontitis as a manifestation of systemic disease). The 2017 World Workshop on the Classification of Diseases and Conditions of the Periodontium and Surrounding Implants revised this system, in evidence that chronic, aggressive and necrotizing forms of periodontitis have identical etiology and pathogenesis, and therefore it was decided to revise the nomenclature to classify all these conditions are manifestations of periodontitis. Phenotypic differences are still recognized in the current (2017) classification system, with localized aggression now being described as a “molar incisor pattern” (molar incisor pattern). Genetics are believed to explain most of the differences in clinical presentation and disease severity between what was previously described as chronic or acute periodontitis.
A literature review conducted in March 2021 using MEDLINE/PubMed did not find any description of patients presenting with both ancloglossia and periodontitis in previous articles. Accordingly, the authors describe three sisters who inherited ankyloglossia and incisive form of periodontitis on the maternal side.
Case examples
Patient 1
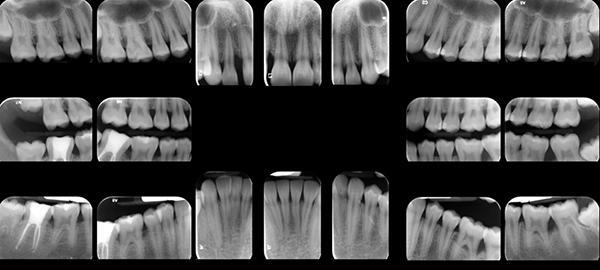
An apparently healthy 19-year-old African American patient presented to the Graduate Periodontology Clinic at the University at Buffalo School of Dental Medicine (PG clinic) for an examination. Her medical history was unremarkable. There was no history of smoking, diabetes, or other systemic disease, the patient denied medication or drug use, and her vital signs were normal. She had no major complaints but was aware of her periodontal condition from a previous dental examination which revealed minimal plaque combined with generalized periodontal pockets 5 mm deep on probing, mainly in the area of teeth 2.6, 2.7, 3.7, 4.6. During the examination, no mobility of these teeth or cracks in the furcation area was found, when probing in 11.8% of cases, bleeding appeared in the studied areas of the gums around the teeth, and there were no gum recessions. X-ray examination revealed slight horizontal bone loss in the region of the posterior and anterior teeth, and an area of vertical bone resorption was also found in the mesial wall of tooth 2.6 (Figure 1). There was no history of restorative dental treatment.
Photo 1. A series of intraoral radiographs of patient 1 is shown. -parodontita-fb8d9fa.jpg” alt=”Hereditary manifestation of ankyloglossia and localized periodontitis1″ />
Her mother, who accompanied the patient during her visit to the periodontist, reported that her daughter had previously been treated for ankyloglossia with a frenectomy procedure at the age of 1 year due to the difficulties of breastfeeding at the time. The patient was diagnosed with a periodontal diagnosis of the presence of localized periodontitis stage III, molar incisor model, grade C12.
Patient 2
This clinical case presents a healthy 17-year-old African-American woman and the middle sister of patient 1, who subsequently came to the clinic after graduation for orthodontic treatment and to close the diastema between two permanent incisors. The patient's mother reported that her daughter was diagnosed with Attention Deficit/Hyperactivity Disorder (ADHD) and was taking methylphenidate 27 mg daily and clonidine 0.1 mg daily. Otherwise, the medical history was unremarkable, the patient was not taking any other medications, and vital signs were within normal limits.
When examining the condition of the periodontium, a minimal accumulation of plaque was noted, but at the same time, the presence of multiple periodontal pockets from 4 mm to 8 mm deep was noted, which were localized primarily in the area of the teeth: 1.6., 1.2., 2.6., 2.7. ,3.7.,3.6., 4.7. On teeth 1.2 and 3.6, I degree of mobility was noted. Root damage in the area of furcation was noted on teeth 2.6., 2.7., 3.7, 4.6. A purulent discharge was found in the area of teeth 1.2., 3.6. The bleeding test during probing was 10.7%, there was no gingival recession.
During the history taking, the patient's mother reported that her daughter in this case had previously suffered from ankyloglossia and was treated operatively with a frenectomy at the age of 11 years. The patient's mother also noted that the frenectomy procedure was performed later than in the case of her older sister (Case 1) because ankyloglossia had no effect on breastfeeding in this case. A review of radiographs revealed moderate horizontal bone loss in the region of the molars and incisors, as well as vertical bone loss mesial to teeth 1.2., 2.7., 4.6. and distal to teeth 3.6., 4.6. (photo 2). Multiple restorations were identified on the teeth, tooth 4.7. was treated endodontically
After clinical examination, the diagnosis of localized periodontitis, stage III, molar incisor model, grade C12 was established.
Photo 2. A series of intraoral x-rays of patient 2 is shown.
Patient 3
Patient 3, a healthy 15-year-old African American female patient and the younger sister of patients 1 and 2, subsequently presented to the clinic with a primary complaint of being upset with her “tongue-tiedness” and wanting to treat it. The patient's mother reported that her daughter had previously been diagnosed with ADHD and was currently taking methylphenidate 27 mg daily and clonidine 0.1 mg daily, but otherwise had an unremarkable history. The patient was not taking any other medications and her vital signs were within normal limits.
During the examination, a minimal accumulation of plaque was noted, but the presence of multiple periodontal pockets was also noted, their depth during probing ranged from 4 mm to 10 mm and they were localized in the area of teeth 1.6., 2.6., 3.7., 3.6. and 4.7. On teeth 3.6., 2.7. mobility of the first degree was revealed, and a root lesion in the area of the furcation of the second degree was detected on the mesial wall of the tooth 1.6. The gingival bleeding test during probing was positive in 28% of cases, and gingival exposure was also found on the lingual side of the lower incisors by 1 mm. A review of radiographs revealed horizontal bone loss in the region of the posterior group of teeth and incisors, and vertical bone loss mesial to teeth 1.6. and 3.6. (photo 3).
Photo 3. A series of intraoral images of patient 3 is presented. -parodontita-a9b181c.jpg” alt=”Hereditary manifestation of ankyloglossia and localized periodontitis3″ />
Further examination revealed ankyloglossia of the frenum of the tongue (photo 4), class II (moderate) according to the classification, which estimates the total movement of the tongue at 10 mm. A diagnosis of localized periodontitis, stage III, molar incisor model, grade C, was established, as well as the presence of deformities of the gingival mucosa and the condition around the teeth (aberrant frenulum).
Photo 4. Ankyloglossia demonstrated in the case of Patient 3.

Treatment
Due to bone loss in the molar/incisor area, the treatment plan proposed for all three sisters consisted of instructions for oral hygiene, scaling and root curettage in combination with systemic antibiotics (500 mg amoxicillin and 250 mg metronidazole three times per day for 7 days), followed by a re-examination of the periodontium after 4-6 weeks. Depending on the patient's response to initial therapy, further alternative treatment options that should be considered will include periodontal maintenance or periodontal surgery aimed at tissue regeneration.
When re-examining the periodontium 4 weeks after the start of therapy, all three patients showed poor compliance with the rules of oral care at home. Moreover, each sister admitted that they did not receive or take antibiotics as prescribed. Not surprisingly, there was no improvement in terms of reduction in the depth of periodontal pockets on probing or the amount of gingival bleeding on probing. Therefore, the importance of excellent plaque control and good hygiene practices to reduce disease symptoms was again explained to patients and instructions were given for home oral care.
The ankyloglossia in patient 3 was surgically corrected by a frenectomy procedure using a 15c scalpel. After administration of 2% lidocaine with epinephrine at a ratio of 1:100,000, the frenulum was completely excised, and 5-0 absorbable chromium thread sutures were placed both on the floor of the oral cavity and on the ventral part of the tongue. During the postoperative examination after 1 week (photo 5), the intervention site healed well, the patient had no symptoms and complaints. Normal tongue function appeared to have been restored, and both the patient and her mother were satisfied with the resolution of the problem. Unfortunately, all patients were unable to return to the clinic for follow-up monitoring and periodontal treatment, despite repeated attempts to reschedule the visit.
Photo 5. The condition of the mucous membrane of patient 3 after the surgical intervention to correct ankyloglossia, illustrated earlier in Photo 4.

Talk
Ankyloglossia is believed to be a familial disorder inherited both in an autosomal dominant and autosomal recessive manner. Although ankyloglossia usually presents as an isolated condition, it can be associated with certain syndromes such as anomalies of missing mandibular incisors, gastrointestinal anomalies, and cleft lip and palate. However, no one seems to have previously described the association between ankyloglossia and periodontal disease.
All three daughters described in this article were diagnosed with stage III localized periodontitis based on evidence of bone loss in excess of that associated with the existing minimal amount of biofilm deposition, and also because of the pattern of bone loss in the molar/incisor area. Such a clinical picture is also considered as an indirect sign of the rapid progression of the disease, corresponding to the classification of periodontal diseases grade C. A family history of periodontitis may also indicate in favor of grade C according to this classification. In this case, all three daughters presented in this article had only one maternal parent, and their mother verbally confirmed a personal family history of periodontitis and ankyloglossia, again confirming the classification of periodontitis grade C for patients 1, 2, and 3. In addition, all sisters from the same ecological and social environment, so they have the same risk factors for developing periodontal disease, in addition to their common parent on the maternal side, this may collectively contribute to the development of their common diagnosis of periodontitis.
Conclusion
This article describes a unique clinical case of three sisters suffering from both ankyloglossia and periodontitis. However, it is not known whether there is a genetic link between ankyloglossia and an increased risk of molar incisor periodontitis, or whether the observed association between ankyloglossia and periodontitis is unique to this family. Therefore, to further elucidate whether common genetic factors contribute to the pathogenesis of these conditions, further studies will be conducted in patients with a well-examined periodontium and a carefully examined medical history.
Authors:
Hajer A. Aldulaijan, BDS, MS
Shahad B. Alsharif, BDS, MS
Robert E. Cohen, DDS, MS, PhD
Lisa M. Yerke, DDS, MS