
A series of cases have been described that prove that COVID-19 survivors may be at risk of developing spontaneous osteonecrosis. Following SARS-CoV-2 infection, these are the first reported cases of osteonecrosis of the jaw.
Between January and August 2021, 12 patients who were prescribed corticosteroids for the treatment of COVID-19 developed spontaneous osteonecrosis of the maxilla. All patients had at least one comorbidity and developed serious bone disease within weeks of testing negative for SARS-CoV-2.
“As the incidence of COVID-19 rises, general dentists and oral and maxillofacial surgeons must be best prepared for the early detection and prevention of PC-RONJ (Osteonecrosis of the Jaw Associated with COVID-19) to avoid irreversible deformity,” write the authors. led by Yehia El-Mahallawi of Alexandria University in Egypt.
12 patients with confirmed SARS-CoV-2
Between January and August 2021, 12 patients were referred to the Oral and Maxillofacial Surgery Department for oral health consultations. Each patient was confirmed positive in a polymerase chain reaction (PCR) test for SARS-CoV-2.
The patients, who included seven women and five men, had a mean age of about 56 years and experienced intraoral manifestations with usual and unusual clinical behavior. Of the patients, five were hospitalized for various periods of time. The rest were treated in home isolation.
Corticosteroids were prescribed for each patient as a treatment for COVID-19. While five hospitalized patients were given dexamethasone 6 mg every 24 hours for 10 days, those in isolation received dexamethasone 6 mg orally for 10 days as well.
None of the patients reported any history of radiation therapy to the head and neck or use of bisphosphonates or other antiresorptive or antiangiogenic drugs. All patients had diabetes mellitus.
After varying duration of COVID-19 disease and its treatment, each patient had a general clinical picture and spontaneous, unprovoked osteonecrosis of the maxilla. The median time they developed jaw necrosis was three to 12 weeks from the day of a negative PCR test.
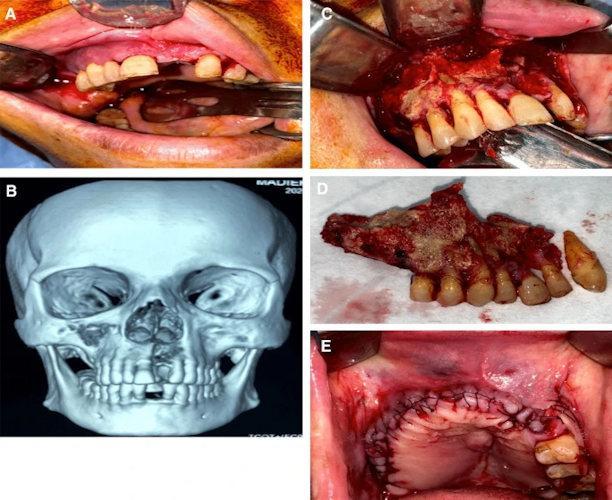
A case of osteonecrosis of the jaw associated with post-COVID-19. A. The image shows multiple maxillary buccal fistulas oozing pus. B. Volume 3D CT rendering showing a necrotic segment of the right maxilla extending to the right maxillary sinus and to the maxillary left lateral incisor. C. Exposed necrotic bone through a striated incision. D. Length of the resected jaw segment. E. Degree of postoperative defect after wound closure.
Nine patients had a mobile dentoalveolar segment of the upper jaw. In addition, a purulent fistula was found in eight patients, palatal edema was observed in three patients, and exposed necrotic bone with mucosal ulceration was found in four patients.
A variant of the clinical presentation that may be present in patients with osteonecrosis of the jaw associated with COVID-19. A. Movable maxillary dentoalveolar segment with intact bony covering of the mucosa. B. Swelling of the palate. C. Ulceration of the mucous membrane and exposed necrotic bone.

All patients underwent computed tomography (CT) to determine the extent of infection. Laboratory tests were not positive for fungal growth, but nine patients were positive for ampicillin- and sulbactam-resistant bacilli, and three others were positive for Enterococcus spp, Neisseria spp, and Staphylococci.
After discussing the treatment with the patients, all underwent surgical debridement followed by removal of sharp bone edges (alveolectomy), copious saline irrigation, and suturing. They then took antibiotics for three weeks.
The patients were observed for at least two months. No recurrence or spread of inflammatory processes was reported. In all cases, a recurring histopathological pattern with patchy tissue was reported. These are bone trabeculae containing numerous necrotic fragments and empty lacunae of osteocytes. A strong infiltration of inflammatory cells was found in the bone marrow, as well as areas of hemorrhage and dystrophic calcification.